METAFIX
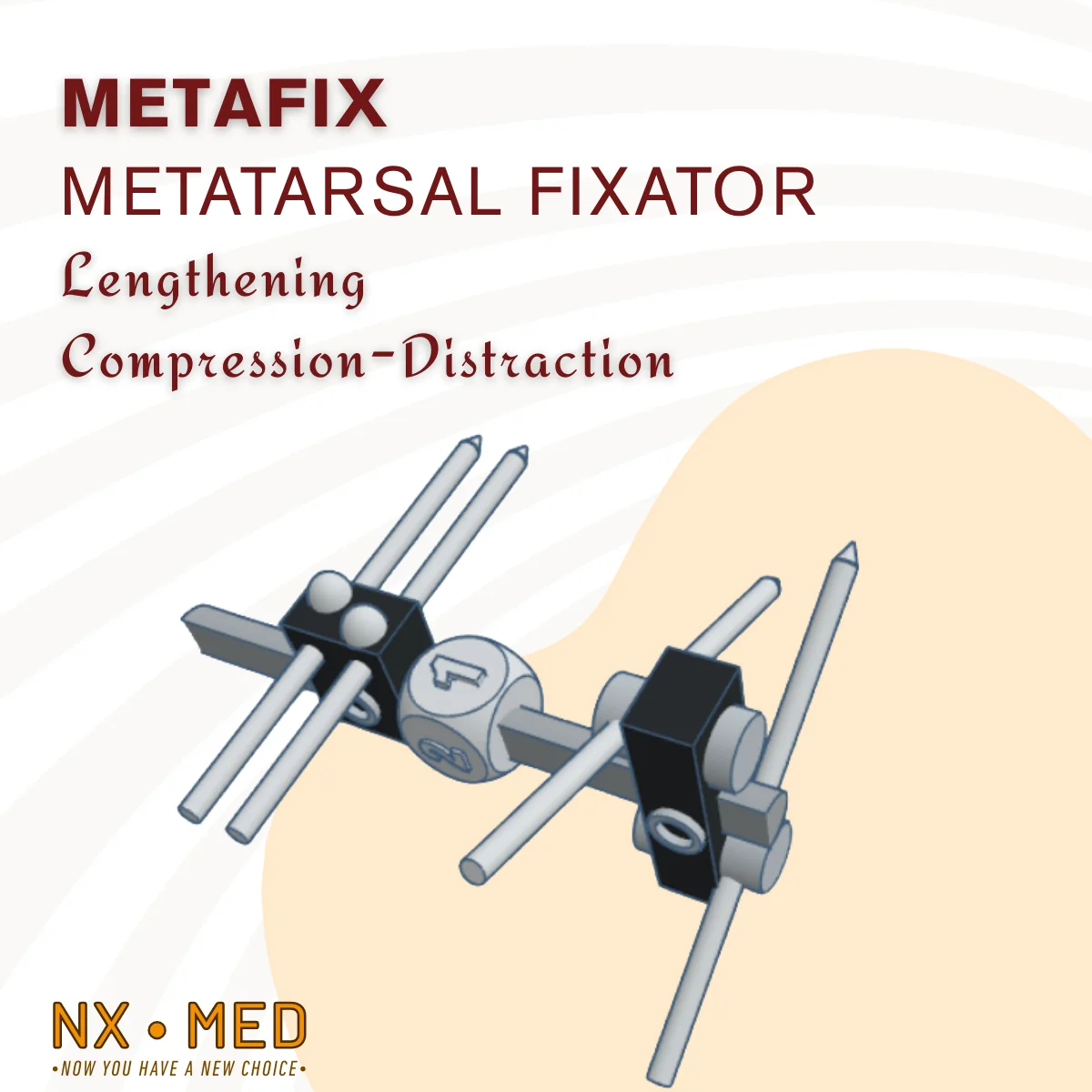
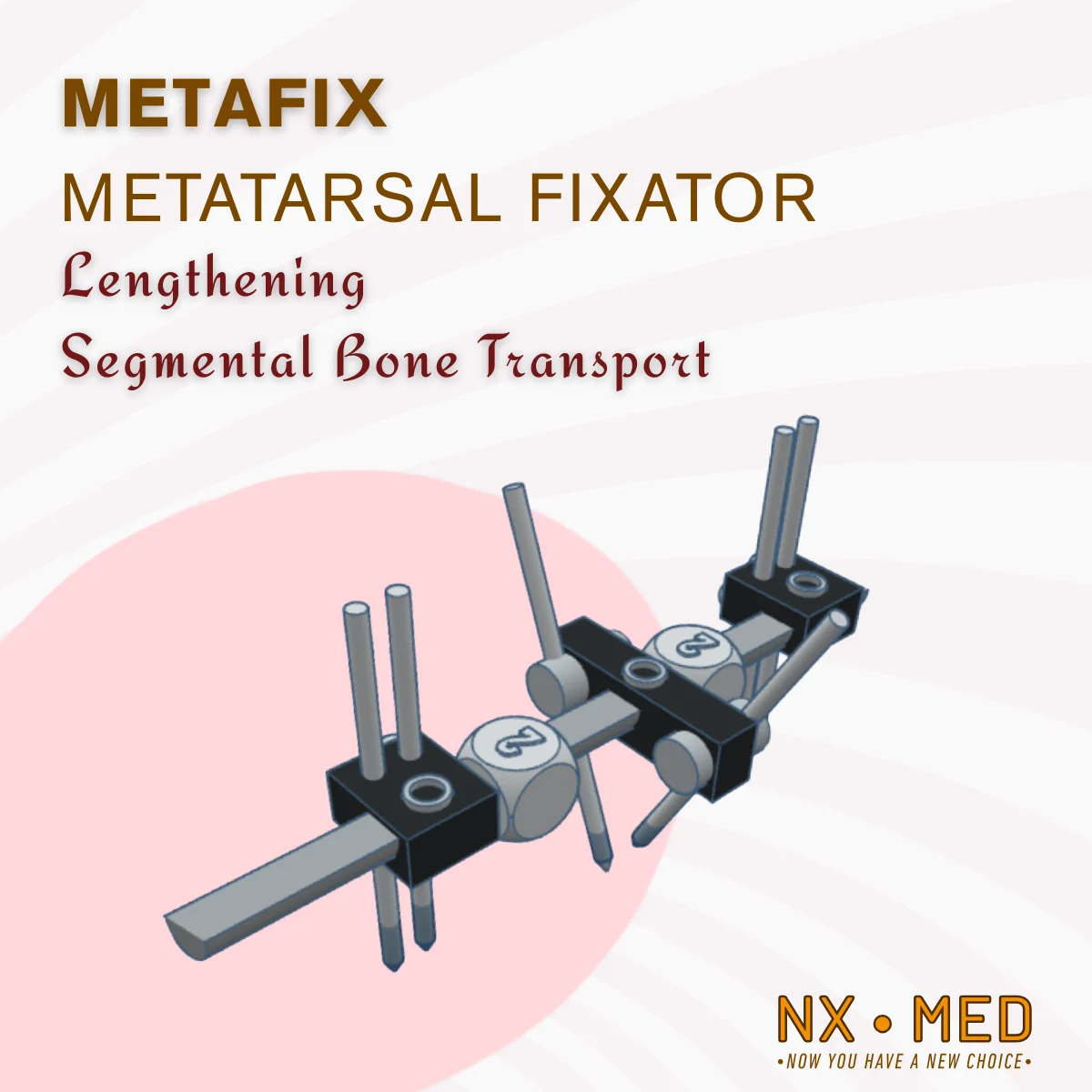
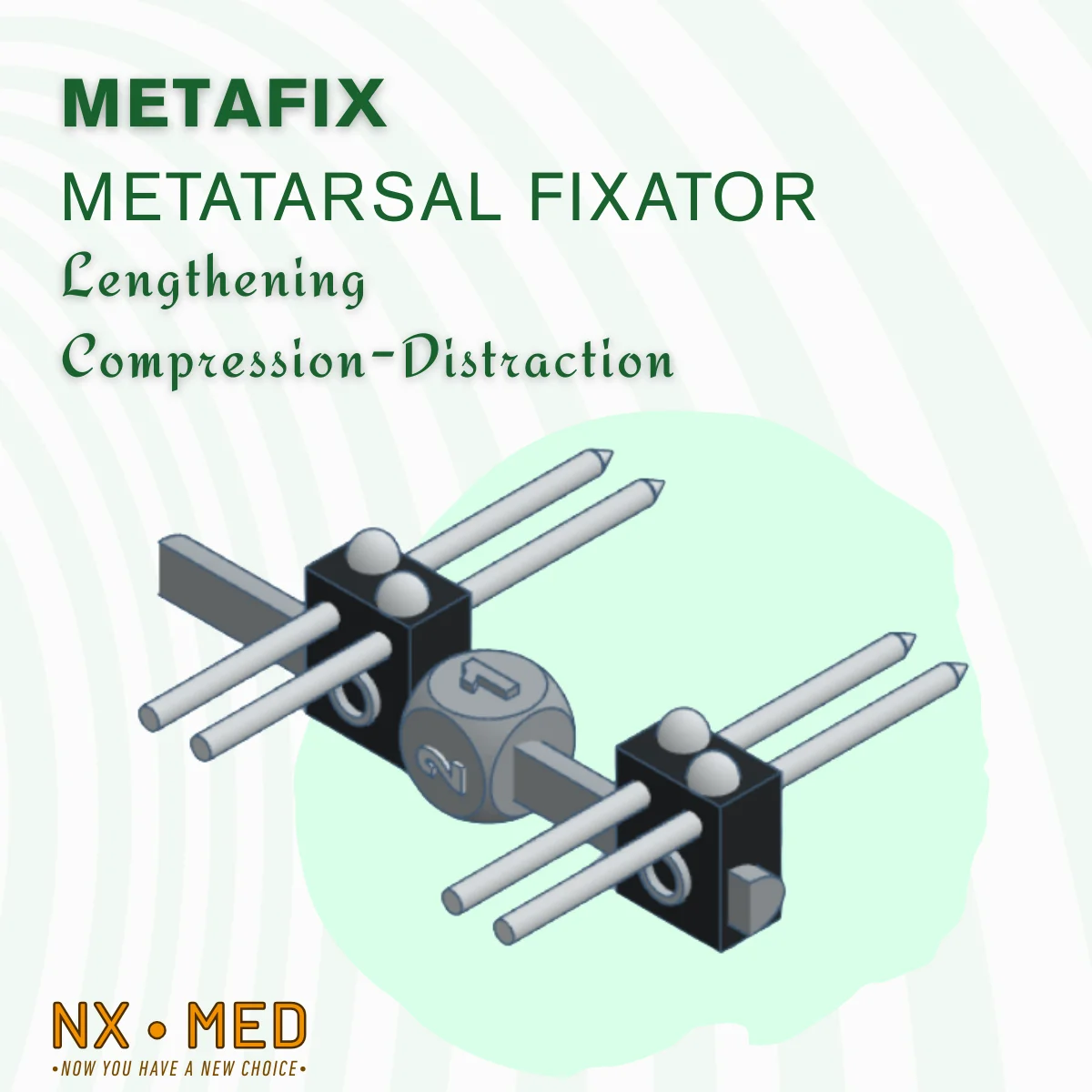
Monoplanar Compression-Distraction External Fixators are widely used and offer superior features, particularly for pathologies of the tarsal and metatarsal bones. For this reason, they are sometimes the primary choice and sometimes the sole option, acting as a surgeon's rescue.
Cannulated compression screws and specially shaped plates are frequently preferred for indications of tarsal and metatarsal bone fractures and deformities.
However, in the following cases, External Fixators should be chosen first:
- Metatarsal Shortness (Brachymetatarsia)
- Distraction Arthroplasty for Hallux Rigidus
- Failed 1st Metatarsal Joint Fusions and Tarsal Joint Fusions
- Metatarsal Pseudarthrosis (Especially the 5th Metatarsal Base)
- Lapidus Procedure for Hallux Valgus (1st Metatarso Cuneiform Arthrodesis)
- Tarsal or Metatarsal Deformities in the Diabetic Foot
- Tarsal or Metatarsal Deformities of Charcot Arthropathy
- Tarsal Fractures Due to Gunshot Wounds
- High-Energy and Open Tarso-Metatarsal Complex Fractures
- Active Tarsal or Metatarsal Infection and/or Osteomyelitis
The advantages of treating these pathologies with an external fixator are as follows:
- It is minimally invasive.
- It can be used safely in patients with infection or high-risk patients.
- Gradual Compression or Gradual Distraction can be performed. Deformity intervention can also be performed after the surgical procedure. These procedures are performed while the patient is in bed, without any need of anesthesia.
- The rate of fracture union and fusion is greater than 95% with fixators featuring distraction-compression properties.
- Because fixation rigidity is generally sufficient, the patient can bear weight early.
- After healing, the external fixator can be easily removed in an outpatient setting, leaving no implant behind.
Challenges and risks of using an external fixator:
- The presence of a relatively bulky device outside the body: Most patients initially complain about this, but they quickly adapt.
- Pin site infection: Superficial soft tissue infection and serous discharge occur at the skin entry points of transmission screws in nearly half of patients. To both prevent and treat this, the pin sites must be kept clean and regular maintenance is necessary. Antibiotics are rarely required. The likelihood of a serious infection requiring fixator removal is very low.
- Pin failure: If a pin with a smaller diameter than necessary is used, the pins may bend or break after loading. The pin diameter should be proportional to the diameter of the bone being used. If the pin is larger than 30% of the bone diameter, there is a risk of bone fracture. If it is smaller than 20% of the bone diameter, there is a risk of pin bending or breakage. The ideal size is around 25% of the diameter of the bone being used.
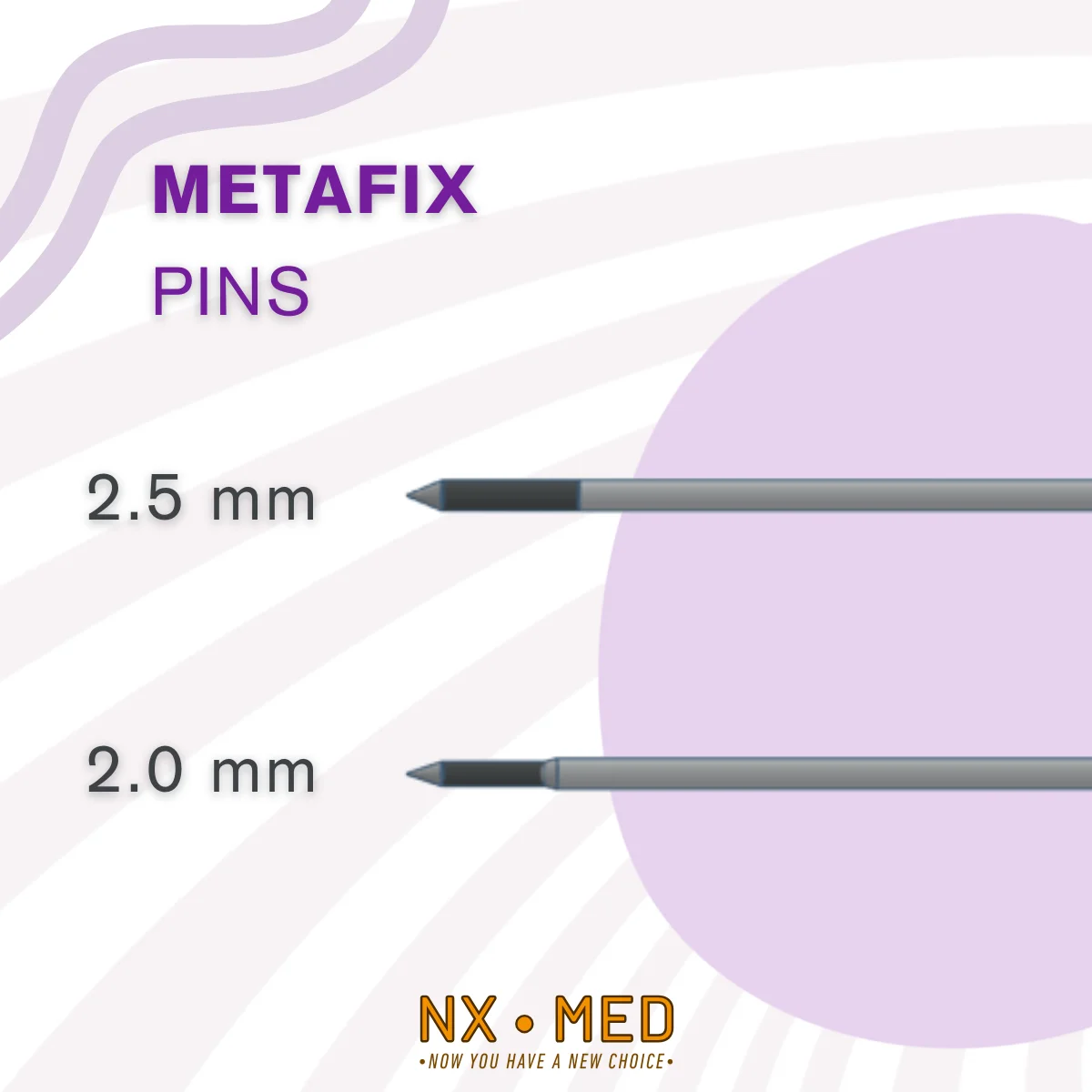
The METAFIX system includes pins in two diameters for external fixation surgery. Their appropriate applications are listed below:
- Ø 2.5 mm – 1st phalanx, 1st metatarsal, other metatarsal bases, and tarsal bones
- Ø 2.0 mm – 2nd, 3rd, 4th, and 5th metatarsal bodies also proximal phalanges
RESULTS AND PATIENT SATISFACTION
Clinical studies have proven that monoplanar rail-type fixators in foot surgery provide early mobilization and high fusion rates. They offer unique features in some indications.
The average fixation period for tarsal and metatarsal pathologies is 8 weeks. Most patients begin weightbearing within 1 week and tolerate it well.
The postoperative period should be supported by physical therapy. The risk of complications is quite low, and the vast majority of patients achieve full functional recovery. Pain and discomfort are minimal, and satisfaction levels are quite high.
The Metafix External Fixator is a new, versatile, adjustable, reliable solution for orthopedic foot surgery that prioritizes patient comfort. It can be used in a wide range of indications and aims to become an indispensable component of minimally invasive approaches in modern foot surgery.