Meniscal Repair
Meniscal repair is a commonly performed orthopedic procedure that involves the stitching or wiring of the meniscus, a crescent-shaped, semi-circular cartilage structure in the knee. It is often used to treat a torn meniscus, which can cause pain, swelling, and locking of the knee joint due to abnormally tracking forces on the knee during movement. Meniscal repair techniques vary depending on the area and type of tear, but typically involve arthroscopic removal of damaged tissue followed by sewing or tacking back together healthy edges of the meniscus using sutures or bioabsorbable material. While minimally invasive surgeries such as laparoscopy are increasingly becoming more common for this procedure, rather than open surgery, most patients can expect to spend one night in hospital and return home with crutches. In addition to taking it easy whilst recovering from their procedure, physical rehabilitative therapy will also be recommended and monitored by their doctor in order for optimal results.
Meniscal Anatomy
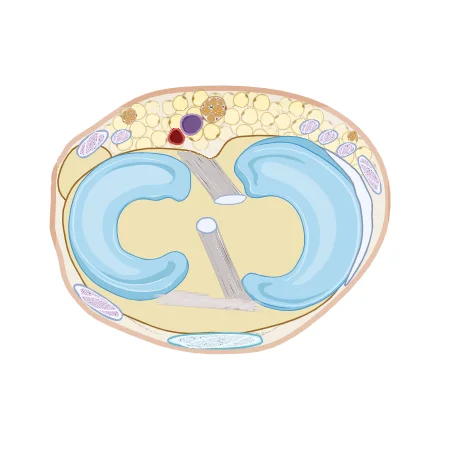
Each meniscus has an appearance like a horseshoe, and is positioned between the bones femur and tibia.
They act as the suspensors and stabilzators of the knee joint. Meniscus and cross section regional structures are as the picture following.
Meniscal Zones
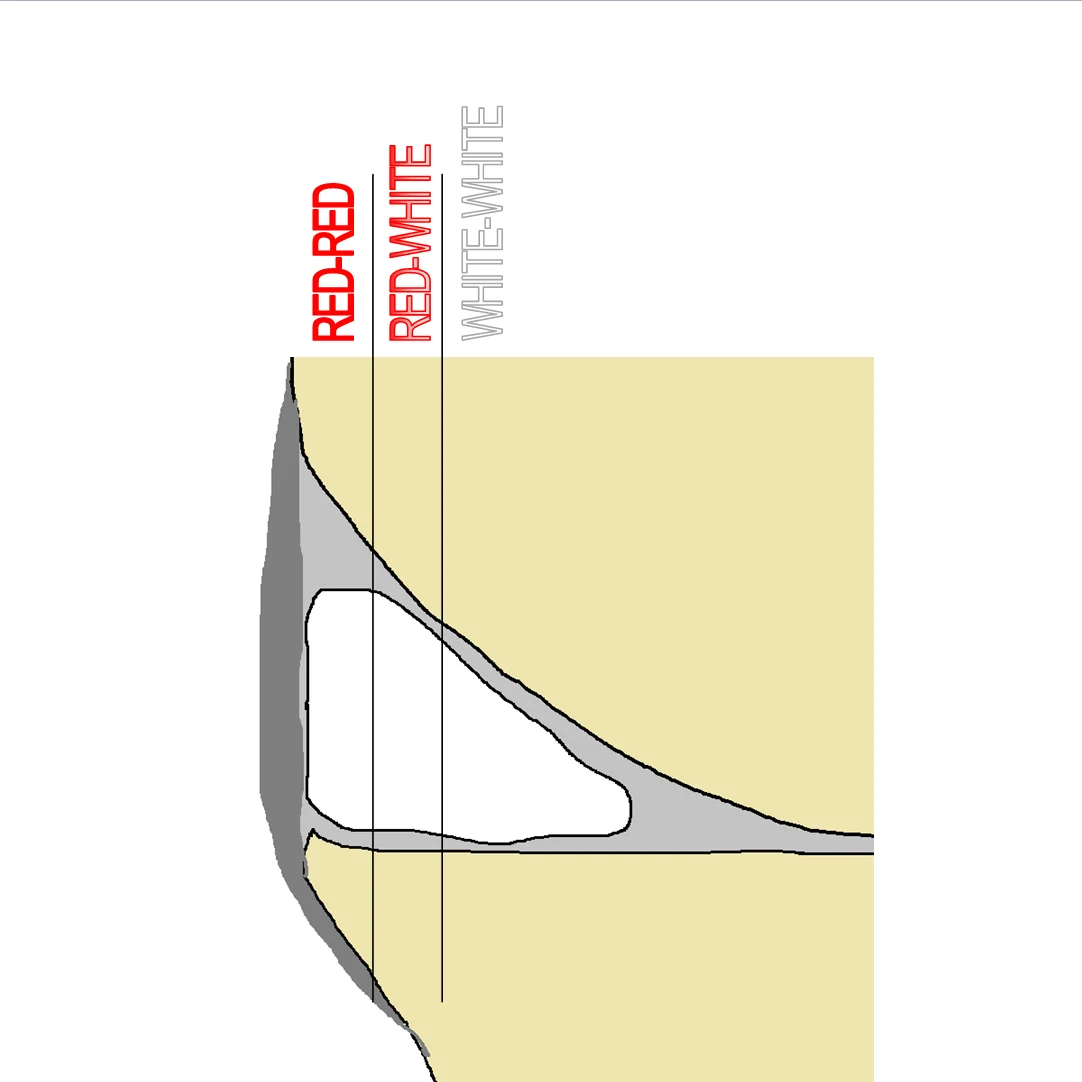
Meniscal section have 3 hystologic zones.
- RED-RED ZONE
Periferic zone have vascularization and have maximum healing potantial.
Important: Tears of this zone have strong indication of suturing due to high healing potential.
- RED-WHITE ZONE
Intermediate zone have no vascularization but have some healing potential. This zone named RED-WHITE zone. Tears of this zone may have indication of repair. But have less success rate.
- WHITE-WHITE ZONE
Medial zone have no vascularization and have minimal healing capacity. Tears of this zone have indication of suturing only at some very special conditions. Resection of this zone is main surgical treatment technique.
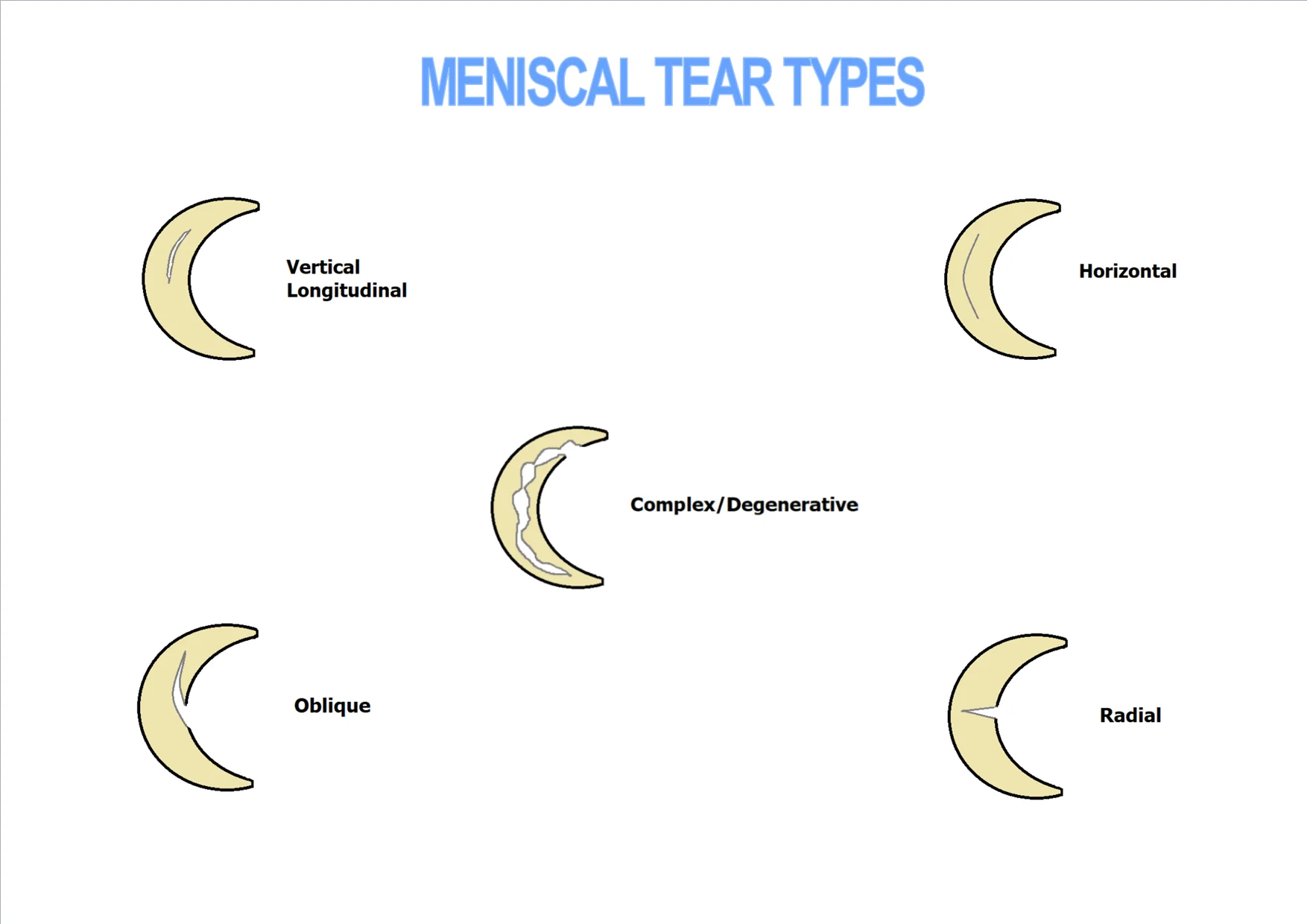
Meniscal Tear Diagnosis
Meniscal tears have 2 main causes.
Traumatic:
This type meniscal tears are acute injuries and mostly due to sport activities. They are mostly need surgical treatment. They should be repair with suturing in order to type of the tear.
Degenerative:
This type meniscal tears are due to chronic degenerative disease of the knee joint. They are rarely indicated surgical treatment. Resection is the main surgical choice of this type. Repair and suturing techniques are not recommend for this degenerative group.
After physical axamination the MR Imagination is the main diagnosis tool for meniscal tears.
Radiology: Grading of meniscal tears at MR imagines are as follows:
This means “Normal Meniscus” as clinically.
Grade II: No links observed with neighboring joint components, though an elevated signal present inside a meniscus. May be horizontal or linear in orientation.
This means “Minimal Meniscal Degeneration” as clinically.
Grade III: Increased intra-meniscal signal intensity with contour to articular surface. May be associated with displacement of meniscal fragments or superficial step formation.
This means “Meniscal Tear” as clinically.
Grade IV: Multiple disruption of meniscal surfaces.
This means “Complex or Degenerative Meniscal Tear” as clinically.
Meniscal Repair Techniques
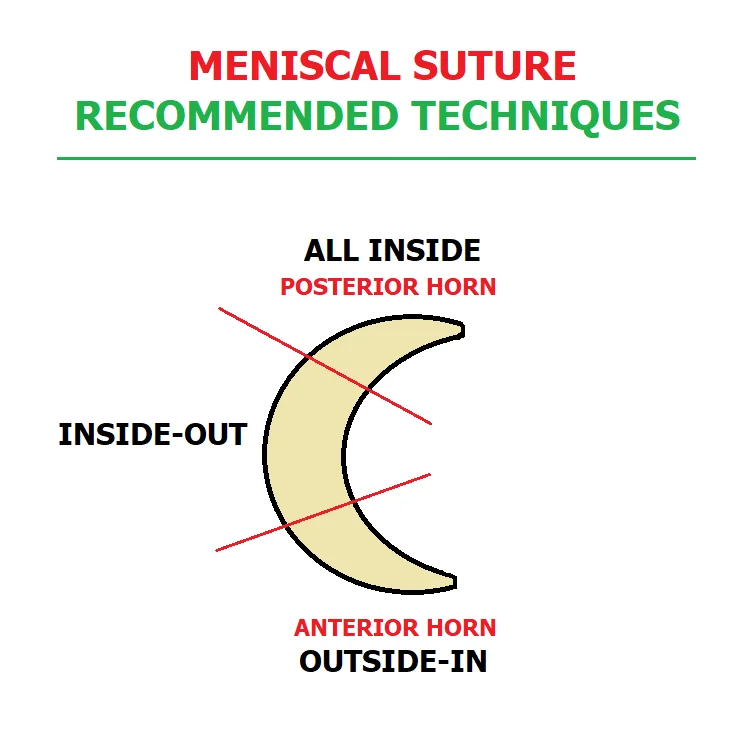
The type of surgery is largely dependent on the type of tear and its location.
The surgical repair of the meniscus have better result than a partial meniscectomy. But the patient need rehabilitation quite a long time.
Meniscal repairs can be performed by the following techniques.
- Open
- Inside-out
- Outside-in
- All-inside.
Open technique is not widely use nowadays. Meniscus repair is mostly perform with arthroscopic visualization, as an inside-out, or outside-in or even the all-inside technique.
Before suturing the tear, debridement should be apply. For each operation they have to remove the loose parts, both surfaces of the tear should be revitalize and the vascularity should be stimulate.
Technique: Should be chosen according to the patient individually.
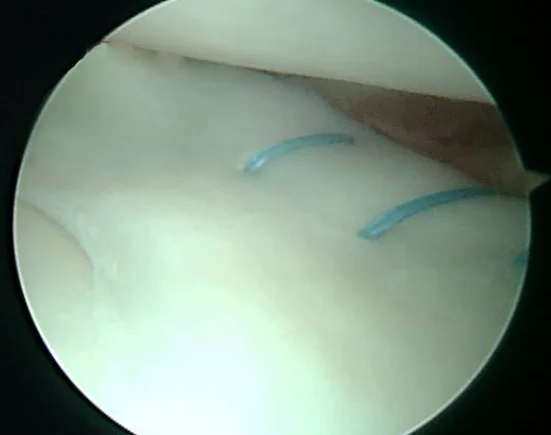
Inside-Out Meniscal Repair Technique
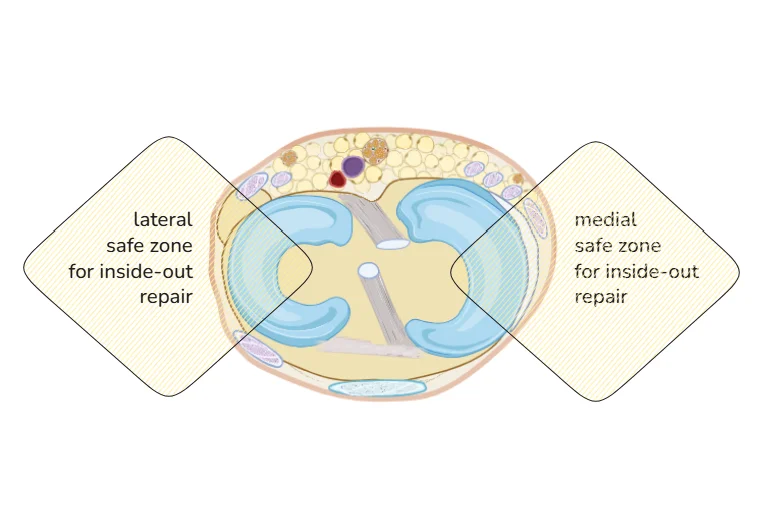
This technique use commonly for tears of the body of the meniscus and partially posterior horn. Especially for Red-Red zone tears Inside-Out technique is strongly recommend to repair the meniscus.
Nonabsorbable No:2/0 loop fiber sutures are using with long flexible needles. It is passed from inside the knee to a protected area on the outside of the joint capsule. The sutures are retrieved through an extra-articular posteromedial or posterolateral incision. If the suturing is performed at the posterior zone than safe are the posterior neurovascular structures should be protected with a retractor. The knots are tied outside of the joint capsule.
This technique is the gold standard for meniscus repair because of the proven long term results, but have a risk of neurovascular complications for posterior horn tears.
It is cost effective and very simple technique with a quite strong fixation stability.
All-Inside Meniscal Repair Technique
This technique mainly can be used for repairing extreme posterior horn tears.
The newest devices are the self-adjusting suture devices. They are based on the same principle as the other devices. An anchor is positioned behind the capsule and a suture compresses and holds the axial meniscal part by using a sliding knot.
These implants share the potential ability to deform and move with the meniscus during weight bearing and carry a lower risk of chondral abrasion. The devices are RapidLoc, FasT-Fix and the Meniscal Cinch.
The advantages of all-inside repair include ease of use, avoidance of an accessory incision, shorter operation time, less risk to neurovascular structures and especially for the suture devices better strength.
The all-inside techniques are attractive. Because all-inside suture kits decrease the operation time.
Outside-In Meniscal Repair Technique
This technique is used for suturing the anterior horn of the meniscus. It is initially designed to decrease the risk of neurovascular complications.
A cannulated 18-gauge spinal needle is passed across the tear from the outside-in. Once the sharp tip of the needle is in view, the suture is passed through the arthroscopic ipsilateral portal. An interference knot is tied in the end of the suture and the suture is pulled back. The process is repeated and the free ends are tied two by two over the capsule through an accessory skin incision until the tear is stabilised.
Outside-In technique: Recommended mostly for anterior horn tears.
Treatment Decision Making
The decision making about a lesion is treated surgically or non-surgically is the first decision made after definitively diagnosing a meniscal tear.
- Patients factors (age, co-morbidities and compliance)
- Tear characteristics (location of the tear, age of the tear and pattern of the tear)
- Tear is stable or unstable.
- Related injuries
Surgical Treatment Indications:
- Unstable meniscal tear.
- Complete or large incomplete longitudinal tear of the medial and lateral meniscus close to the base.
- Large flap tear.
- Bucked-handle tear.
- Nonoperative treatment is rarely successful in treating meniscal tears of young athletes and the repair of the torn menisci is often required.
Nonoperative Treatment Indications:
- Degenerative Tears
- Asymptomatic stable tears
- Contraindications of Meniscal Repair:
- Degenerative Meniscal Tissue
- Knee Joint Instability
- Complex Tears
- Radial Tears of central avascular region
- Gonarthrosis
- Joint infection
- Local skin disorders
Important: In case of ACL rupture or any other ligament instability should be reconstructed with meniscal tear suturing surgery..
Results
Outcome Measures:
Vertical and Horizontal tear types are most likely to repair. The Radial and Oblique types are less likely to repair. Complex or Degenerative tears have no repair indication with sutures.
An overall meniscal repair success rate %60-80 according to applying to the correct type, technique and patient.
There is no change in outcome for those who receive meniscal repair based on age or amount of time passed since initial incident.
If vertical tears are wide they can dislocate inside the joint cartilage and may cause locking of the knee joint. This dislocated type vertical tears specifically named as “bucket-handle tear”.
As a special indication, isolated locked bucket-handle meniscal tears are healing at a high rate when repaired suturing; even when the tear is in the white - white zone.
Complications:
Complication rate is %1-2 of the surgical repair of meniscal tears. These complications include; Hemarthrosis, infection, thromboembolic disease, anesthetic complications, instrument failure, reflex sympathetic dystrophy, ligament injury, fracture and neurologic injuries. With hemarthrosis being the most common complication and neurologic injuries are very rare. No vascular injuries were reported.
Conclusion: Meniscus tears should be repaired in every patient where indicated.